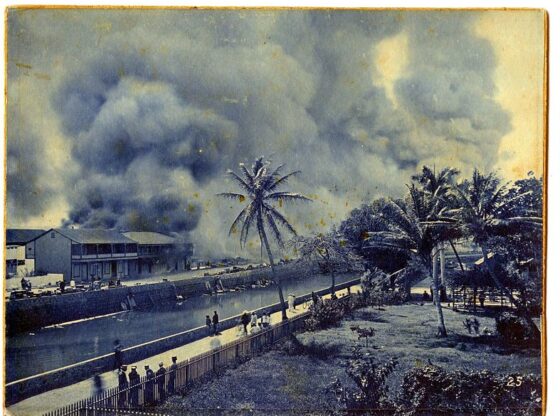
 Honolulu Chinatown Fire of 1900. Photo by Gabriel Bertram Bellinghausen, via wikicommons
Honolulu Chinatown Fire of 1900. Photo by Gabriel Bertram Bellinghausen, via wikicommons By Michael G. Vann
As individuals around the world faced unprecedented government ordered lockdowns to flatten the curve of spread of COVID-19, many of us turned to the safety of books. One of the few bright spots of 2020, at least for those of us privileged enough to shelter-in-place in our home offices, has been a pandemic of reading. This microsyllabus is not extensive or exhaustive but designed to accomplish two specific goals: provide essential information on the histories of pandemics and engage radical critiques of the political, social, and economic contexts of disease outbreaks. As historians, most of us may not have taken many STEM courses and we probably don’t think much about disease cycles, the role of animals in zoonosis, or the fascinating differences between viral and bacterial infections. Thus, this brief list serves as a primer for us to master some of the basics of the history of disease so that we can be better informed and, frankly, not sound foolish when talking with those who are more well-versed in medical issues. Closer to our areas of expertise, this microsyllabus offers readings that should serve as pathways into the historiography of disease, highlighting the ways that crises such as pandemics can reveal the power relationships often hidden behind curtains of Gramscian hegemony.
First, a few words on terminology. What is the difference between endemic, epidemic, and pandemic disease? Really, this is a question of geographic scope. Endemic disease refers to the baseline level of an illness in a given area, essentially a localized disease found in a specific region or regions. An epidemic is when a disease unexpectedly begins to impact a large number of human beings and infects new populations in several areas. A pandemic is when an epidemic disease impacts multiple countries and continents. Think of the transition from endemic to epidemic as a disease achieving some sort of break out and the pandemic state as the subsequent globalization of an epidemic disease. We should not anthropomorphize disease as this is poor scientific thinking and can lead to problematic metaphors. Since diseases do not have agency it is human activity that makes diseases into epidemics and pandemics. When humans come into direct or indirect contact with wild animals that are disease reservoirs, zoonotic diseases can jump from animal hosts into humans. Thus, human encroachment on forests can create a pandemic. The growth of towns and cities had led to epidemics for the simple reason that people living in close proximity spread diseases amongst themselves. The bigger the city, the bigger the risk. Just as epidemics require urban centers, pandemics require global transportation. From the advent of the Silk Roads to the arrival of budget airlines, historically significant developments in long-distance travel have consistently created pandemics. The faster the trip, the bigger the risk. An irony of globalization is the spread of devastating diseases.
Disease outbreaks can be stress tests that reveal a political-economic system’s structural weaknesses. During the first few months of this pandemic we have seen the inability of America’s market-based health care sector to provide sufficient protective gear for first-responders, enough ICU beds for those who have fallen ill, or tests for working people who may have been exposed to COVID-19 (while NBA players, Hollywood celebrities, and politicians seemed to have had no trouble getting tested in the early days of the pandemic). Just as Arundhati Roy declared COVID-19 to be “a portal” history offers numerous examples of diseases serving as a catalyst for historic transformations. Most famous is perhaps the ways in which the 14th century Black Death helped to break feudalism in Western Europe. But that pandemic also weakened the Mongol Yuan Dynasty, leading to the rise of the ethnically Chinese Ming Dynasty and its nativist policies. Perhaps the most devastating examples are the that Old-World pathogens, often arriving via trade routes long before the Iberian conquistadors themselves, destabilized the Aztec and Inca empires and facilitated Spain’s dramatic expansion in the Americas.
Ethnic scapegoating and xenophobic violence frequently erupt during disease outbreaks. Again, the Black Death in Europe serves as the best-known example. Attacks on Jews were common in that late Middle Age pandemic. More recently, during the age of high imperialism, Western medical experts linked Chinese bodies to contagious diseases such as the plague. At the turn of the 20th century, French colonial authorities in Vietnam deemed Chinese to be natural carriers of the plague and thus imposed stricter surveillance of immigrant laborers and merchants from China. In 1900, when faced with a plague outbreak, the white supremacist government burned down Honolulu’s Chinatown. Even though the conflagration may have been an accident, it served as an example to others. The following year municipal authorities in San Francisco quarantined their Chinatown and openly discussed implementing the “Honolulu solution”. As a child in Hawai’i during the 1970s, I recall older members of our family calling leprosy the “Pākē disease,” Pākē being a derogatory term for Chinese. Currently, Donald J. Trump and other xenophobes have gone out of their way to associate the disease with Trump’s favorite rival, China. His flippant use of offensive racist terms such as “Kung Flu”, and its warm reception from his adoring rally attendees, reminds us that pandemics and Sinophobia are frequently intertwined. Viral cellphone videos prove that even in allegedly progressive Northern California such rhetoric has led to a rise in hate crimes against Asian Americans.
Finally, pandemic disease impacts the most vulnerable members of society. Those without the financial means to access health care are hit hardest, as are those that live in insalubrious and cramped housing. Far too often only wealth or class status can guarantee safety. As we see today, while the professional managerial class can work from home, essential (read “required”) services are performed by the lowest paid members of the workforce. Social distancing is a social privilege. Thanks to late capitalism’s structural racism COVID-19 has hit working class Black and Latinx communities disproportionately harder than wealthier white neighborhoods. Due to their historical isolation and contemporary marginalization indigenous communities from the Dakotas to the Amazon are particularly vulnerable (both South Dakota Governor Kristi Noem and Brazilian President Jair Bolsonaro have been disdainful and contemptuous of tribal leaders’ concerns).
This first list offers a selection of essential reading for a baseline knowledge of the history of disease. Reading three or four of these books will ensure that you have the fundamental knowledge base to engage the more the more critical and theoretical books from the second list.
- Mitchell L. Hammond, Epidemics and the Modern World (University of Toronto Press, 2020) is the latest and one of the best all-purpose surveys on the subject. While written as a textbook for classroom use, scholars not well-versed in the history of disease would do well to start here.
- William H. McNeill, Plagues and People (Doubleday, 1977) is one of the first true global histories of disease from a pioneer of the field of world history. While dated, the book remains a classic as McNeill’s argument for disease being a crucial variable in human history was set the paradigm for the historiography of epidemics.
- John Aberth, Plagues in World History (Roman and Little Field, 2011) offers an accessible collection of micro-histories of plague, smallpox, tuberculosis, influence, cholera, and HIV/AIDS. [ https://rowman.com/isbn/9780742557062/plagues-in-world-history ]
- Michael T. Osterholm & Mark Olshaker, Deadliest Enemy: Our War Against Killer Germs (Little, Brown, and Company, 2017), despite embracing the militarist metaphor, offers a clear and extremely well-informed discussion of the recent efforts to use public health measure to combat infectious disease. As one of the United States’ most important epidemiologists, Osterholm offers important insights into how we can best respond to global health threats. This book was written for a general audience and is free of some possibly alienating academic discourses. A new edition is being reissued with a short preface about COVID-19 (in short, his 2020 message is “I told you so”).
- Laurie Garrett, The Coming Plague: Newly Emerging Diseases in a World Out of Balance (Penguin, 1994) is an important study of our current global crisis by a Pulitzer Prize winning journalist. Published 25 years before COVID-19, the work warned us that a newly emerging disease could plunge the new world order into chaos. In her sequel to The Coming Plague, Betrayal of Trust: The Collapse of Global Public Health (Hyperion, 2000), Garrett is remarkably prophetic in regard to the perfect storm created by globalization and neo-liberalism.
- Alfred W. Crosby, The Columbian Exchange: The Biological and Cultural Consequences of 1492 (Greenwood Publishing, 1972) , Ecological Imperialism: The Biological Expansion of Europe, 900-1900 (Cambridge University Press, 1986), and America’s Forgotten Pandemic: The Influenza of 1918 (Cambridge University Press, 1989) are must-reads for all scholars of disease. Despite the discipline’s initial uneasiness with his approach, as seen in a tepid review in The American Historical Review, Crosby helped to create the field of environmental history and coined the term “Columbian Exchange.” Echoing Marx in The 18th Brumaire, Crosby’s work shows the ways in which human beings do have agency but within biological conditions not of their making.
- Thomas J. Bollyky, Plagues and the Paradox of Progress: Why the World is Getting Healthier in Worrisome Ways (The MIT Press, 2018) challenges positivist and technocratic optimism by pointing out that we are currently seeing crises of over-consumption and over-abundance. Considering that the book was put out by the Council on Foreign Relations, it should be treated with a certain degree of skepticism. That said, Bollyky’s critique of neo-liberalism’s impact on public health is worth consideration.
Once you have established a basic framework of the history of disease and public health, the following titles can serve as ways to explore the larger issues in the history of pandemics, beyond a basic framework of the history of disease and public health.
Susan Sontag, Illness as Metaphor and AIDS and its Metaphors (Anchor Books, 1990).
This volume is comprised of two classic essays, but keep in mind that classics often read as dated. While some of the issues Sontag discusses were much more germane to the 1970s (cancer patients hiding their illness out of shame) and the 1980s (the as-yet unknown mysteries of HIV/AIDS inducing panic), her overall argument that we inappropriately assign social meaning to diseases and those who have diseases was paradigm setting at the time and remains relevant today. Obviously, Donald Trump’s generally buffoonish xenophobia and his specifically Sinophobic tweets come to mind. Sontag wrote Illness as Metaphor while recovering from cancer in 1978. In this piece she compares the views of cancer and tuberculosis in Western culture. She persuasively demonstrates the romanticization of tuberculosis contrasts sharply with the horror of cancer. Drawing from a substantial body of literature, this erudite essay describes the ways in which TB patients were seen as sensual creatures with heightened libidos. Their wan looks became fashionable and were aped by many who did not suffer from the disease. Conversely, Sontag discusses how doctors often hid the diagnosis of cancer from the patient, telling only their families and not the afflicted. Illness as Metaphor urges us to reject using diseases as metaphors for unrelated issues. In AIDS and its Metaphors Sontag updates her critique for the new pandemic. Written in the last year of the Reagan era and as contemporary science was only beginning to come to terms with the disease, the essay explores how Americans deployed various social prejudices – including homophobia, class privilege, and anti-Blackness – to judge those with Human Immunodeficiency Virus or Acquired Immunodeficiency Syndrome. Sontag’s main argument is that we need to be more careful with the language we use to talk about disease and people living with disease. While she criticizes the use of specific metaphors, especially those drawn from warfare, she clearly does not want to live in a world without metaphor. Thus, she urges us to be more careful with the language we use when talking about disease. Sontag wants us to talk about disease as a medical issue and not conflate it with larger political meanings. Today as we are faced with Trump’s intentionally provocative use of the phrase “Chinese virus” during his surreal press conferences and yelling “Kung Flu” at his quasi-fascist campaign rallies, Sontag’s warning remains important.
Mike Davis, The Monster at the Door: The Global Threat of Avian Flu (Revised and Expanded) (Owl Books, 2006).
Of course you know Mike Davis’ City of Quartz: Excavating the Future in Los Angeles (Verso, 1990) or perhaps Late Victorian Holocausts: El Niño Famines and the Making of the Third World (Verso, 2000) and you’ve likely read one of his many essays on the various contradictions of late capitalism, so this MacArthur Genius Grant winning author needs no introduction to this audience. Sadly, The Monster at the Door might be one of his most overlooked books. In interviews he has gone on record as being so afraid of the book’s subject that he refuses to keep a copy in his home. Davis, who has self-identified as a “Marxist-Environmentalist”, deftly explains the way in which annual bird migrations bring influenza from Siberian lakes to warmer bodies of water in southern China and Southeast Asia. While this natural cycle has occurred for thousands of years, human activity in the past two centuries has led to avian disease break outs ranging from the seasonal flu to more serious influenza pandemics such as in the 1890s, 1918, 1957, 1968, and 1997, as well as corona viruses such as SARS (Severe Acute Respiratory Syndrome) in 2003. Davis demonstrates that Chinese, as well as South and Southeast Asian, demographic growth and the industrialization of agricultural production have created a perilous situation. Population growth in these parts of Asia has resulted in rapid urbanization, but the lines between city and countryside are not firm. Thus, large business complexes, manufacturing centers, and residential structures can often be found near farms raising ducks and chickens. While it is well known that living in close proximity to poultry and waterfowl facilitates diseases jumping from avian species to humans, Davis notes the even greater danger of factory farms. Singling out Thai chicken production, The Monster at the Door explains that massive chicken farms are extremely vulnerable to infection. Influenza from wild migratory birds can easily get into these communities of caged birds, spreading like wildfire. As people often live near these well-staffed sites and Asia is famous for its so-called “wet markets” with thousands of caged live animals, bird-to-human transmission is facilitated by this inter-species promiscuity. Linking technology and biology, Davis completes his portrait of this epidemiological time bomb with a consideration of the sudden growth in low cost air travel. With the advent of mass tourism in early 21st century China and Southeast Asia, transportation infrastructure can quickly turn an Asian disease event into a global pandemic. It should come as no surprise that this brilliant Marxist thinking ties this impending health crisis to the contradictions of late capitalism. Davis also calls out the Eurocentric bias in the discipline, arguing that far too many historians of disease focus on the impact of the so-called Spanish Flu in Western Europe and the United States of America and ignore its impact on western India where possibly 18,000,000 people died in 1918. Davis warns that the true disaster of the next pandemic will not be in the relatively pampered global north but in the crowded slums of the global south.
Myron Echenberg, Plague Ports: The Global Urban Impact of Bubonic Plague, 1894-1901 (New York University Press, 2007).
Mark Twain allegedly quipped “history doesn’t repeat itself, but it often rhymes”. Whether he actually said it or not, Myron Echenberg’s Plague Ports proves this aphorism true as reading this book now shows many parallels between the COVID-19 pandemic and a global health crisis 120 years ago. This masterful piece of historical research traces the spread of the Bubonic Plague during the most important years of the Third Plague Pandemic (1855-1960). Coming out of mountainous Yunnan in southern China in the late 19th century, the disease was ignored for decades but suddenly received international attention when it arrived in Canton and then Hong Kong in 1894. Because of the British Empire’s imperial infrastructure, which included telegraph lines and steamships, graphic reports of sudden deaths and urban chaos made their way around the world. Meanwhile, French scientists working in Hong Kong and Bombay identified the plague bacillus and rat fleas as the vector in the spread of the disease. Authorities around the world quickly realized that the newly industrialized network of global maritime transportation would spread the disease to all significant seaports. Similar to today’s crisis, the world knew this disease was coming but did not understand how best to prepare for it. Echenberg’s book follows the plague as it hit Hong Kong, Bombay, Alexandria, Porto, Buenos Aires, Honolulu, San Francisco, London, and Cape Town. This comparative history explores how a variety of port cities responded to the crisis, consistently illustrating how race and class structured state responses to the pandemic. In perhaps the most shocking moment of the crisis, the white supremacist colonial government burned down Honolulu’s Chinatown. While the fire may have accidentally gotten out of control and destroyed far more property than initially intended, its results were hailed as a great success and there were calls to enact the “Honolulu solution” when the disease hit San Francisco’s Chinatown. Sinophobic reactions to the pandemic were as common then as they are now. Echenberg does give credit to the brave attempts to establish effective public health regimes in the face of a terrifying and still poorly understood disease. However, he places the origins of public health in the historical context of high imperialism and racism. The author’s Africa in the Time of Cholera: A History of Pandemics from 1817 to the Present (Cambridge, 2012) is also worth reading. While focused on one disease on one continent, Echenberg puts Africa in a global context. Africa in the Time of Cholera is most successful in illustrating how imperial intrusions and post-colonial restraints impacted a range of communities.
Robert Peckham, Epidemics in Modern Asia (Cambridge, 2016).
In contrast to many histories of epidemics, Peckham does not divide this book into a series of micro-histories of individual diseases. Rather, he presents chapters that focus on the human actions that facilitate the spread of disease: mobility, cities, environment, war, and globalization. This is an important conceptual intervention in the historiography as far too many authors run the risk of assigning agency to disease. Germs, viruses, and bacteria do not make decisions. Instead human beings create situations, structures, and processes that allow these organisms to either thrive, whither, or remain constant. By focusing on the 19th and 20th centuries, Peckham’s book shows how the disruptions of Western imperialism, rapid urbanization, prolonged military action, and the industrialization of transportation fostered ecological chaos, resulting in a series of epidemics. The book also explains how states responded to these changing disease ecologies. In addition to this thematic history of disease in modern Asia, Peckham has two anthologies of note: Imperial Contagions: Medicine, Hygiene, and Cultures of Planning in Asia (Hong Kong University Press, 2013) [co-edited with David M. Pomfret] and Empires of Panic: Epidemics and Colonial Anxieties (Hong Kong University Press, 2015). As much of the historiography of disease is Eurocentric, the ways in which these three books center Asia can serve as a crucial corrective.
Seth Archer, Sharks Upon the Land: Colonialism, Indigenous Health, and Culture in Hawai’i, 1778-1855 (Cambridge, 2018).
Archer’s recent study considers the now familiar pattern of virgin field epidemics; when the moments of initial contact introduce disease to previous isolated populations lacking acquired immunological defense systems. As with the Columbian Exchange leading to the massive depopulation of the Americas, Captain Cook’s ships were the first to bring unfamiliar ailments to the Hawaiian Islands in 1778. Following the H.M.S. Resolution and H.M.S. Discovery, a flood of other vessels brought explorers, missionaries, whalers, settler-colonizers, and plantation laborers carrying everything from the common cold to tuberculosis. In the space of roughly three generations, disease killed approximately 90% of the Indigenous population. In addition to shortened lifespans and rising infant mortality rates, sexually transmitted diseases also served to render survivors sterile, further accelerating the demographic collapse. In the face of this horror, Hawaiian culture was thrown into chaos, thus facilitating the rapacious greed of haole colonizers. Foreshadowing Naomi Klein’s “disaster capitalism”, opportunistic Westerners seized the moment and introduced the alien concept of private property. In the Great Māhele (land division) of 1848, the children of New England missionaries and five large sugarcane corporations acquired most of the archipelago’s real estate. Denied access to farmlands and forests for hunting and collecting, surviving kānaka maoli became wage laborers on plantations, ranches, and maritime ports. Such a rapid disposition and proletarianization of the native population would have been impossible without alien diseases tearing apart the indigenous social fabric. Archer’s case-study is commendable for several reasons. Most importantly, his excellent language skills and impressive archival work allow him to bring indigenous voices into the narrative. This stands in sharp contrast to many works on the Columbian Exchange where such sources are nowhere near as plentiful or accessible. Archer shows how the Hawaiian people were not merely passive victims but exercised historical agency and deployed their cultural and medical knowledge in an ultimately failed effort to resist the macro- and micro-biological invasion. Archer shows the ways in which the sudden insertion into the global capitalist economy traumatized Indigenous communities.
AUTHOR BIO
Michael G. Vann is a professor of world history at California State University, Sacramento, where he teaches courses on Southeast Asia, imperialism, epidemic disease, genocide, and the Cold War. His most recent book is The Great Hanoi Rat Hunt: Empire, Disease, and Modernity, in French Colonial Vietnam (Oxford UP, 2018) a surprisingly humorous story of the colonial state’s quixotic campaign of sewer rat eradication and the ways in which the Vietnamese resisted and outsmarted their French overlords during the most dangerous years of the third bubonic plague pandemic. His current research explores representations of Cold War era mass violence in Indonesia, Cambodian, and Vietnamese museums.